
Pancreatic Surgery
Introduction
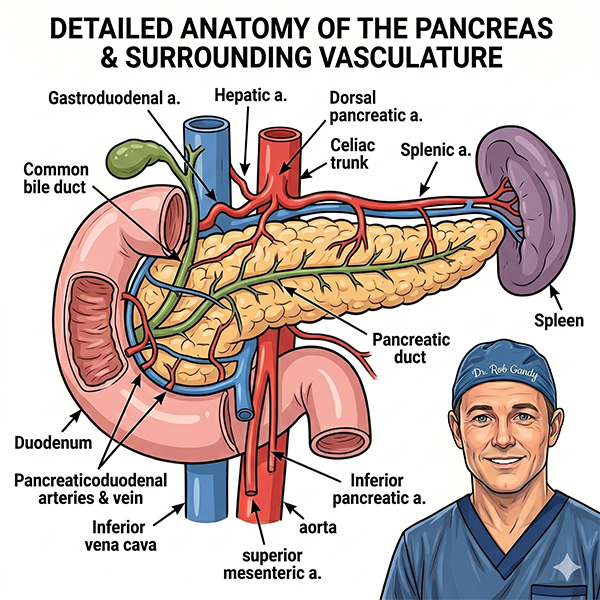
The pancreas is an organ that is located behind the stomach at the back of the abdomen. The pancreas makes hormones that regulate blood sugar (insulin and glucagon) and produce digestive juices that help the body break down food. Tumours from the cells that produce digestive juices are pancreatic cancers (adenocarcinoma). Tumours from the hormone producing cells are pancreatic neuroendocrine tumours.
The position of the pancreas in the back of the abdomen and its relationship to the major blood vessels, the small intestine and the liver, mean that all pancreatic surgery is major and complex. Surgery to the pancreas is best performed by a specialist HPB surgeon.
Why have surgery on the pancreas?
Pancreatic surgery is no small undertaking, both for the patient and the surgeon. The decision to have surgery on the pancreas must be justified and in most cases, is for 3 reasons
- Proven pancreatic cancer (or distal bile duct cancer)
- Pancreatic lumps or cysts that may harbour some cancer or may become cancers, if left untreated.
- Pancreatic neuroendocrine tumours
- Severe scarring of the pancreas (chronic pancreatitis) which may be improved by surgery.
Why have a pancreas operation if cancer can’t be proven with a biopsy?
Pancreas cancers can be difficult to biopsy and in 10-15% of cases biopsy may not be accurate. Biopsy can also injure the pancreas. Only a small proportion of pancreatic cancers are ‘curable” with surgery, so the best chance of long survival is to remove the tumour before it spreads, or even before it becomes cancerous.
Who can have pancreatic surgery?
Only 10-15% of people who have pancreatic cancer can have a pancreas resection (removal). If the cancer has spread, then surgery becomes futile. Radical surgery can be performed if the tumour has spread to adjacent lymph nodes or major blood vessels, but the chances of long term survival decreases. In this setting chemotherapy, can be given prior to surgery to try and improve survival, but in this instance the 30% of tumours will spread prior to the surgery.
What specialist test may be performed prior to surgery?
In addition to blood tests, the anaesthetic doctor may want to assess your fitness for surgery. This is done at the pre-anaesthetic clinic appointment.
Endoscopic ultrasound biopsy – this test is not always undertaken, but is important if you are going to have chemotherapy prior to surgery or if you would prefer a biopsy proven diagnosis.
ERCP– ERCP is performed if the tumour is blocking the bile outflow of the liver. Complications especially bleeding occur if the bile duct is blocked and you are very jaundice.
PET Scan – this is not funded for pancreatic cancer in Australia, but may be useful if there is a suspicion of spread of the tumour prior to surgery.
Laparoscopy – Used to exclude tumour spread to the abdomen, prior to your operation.
Pancreatic Surgery
The decision to perform pancreatic surgery is a complex discussion between you and your doctors. The decisions are based on your health, the extent of your tumour and the risks involved. There are two operations for pancreatic tumours, depending on the location of the tumour.
If on the right side of the pancreas (head or neck) a Whipple’s procedure (pancreatoduodenectomy) is required. This procedure is also performed for duodenal cancer and some bile duct cancers.
If the tumour is in the left side of the pancreas (body or tail) a distal (subtotal) pancreatectomy is required. Removal of this part of the pancreas and the associated blood vessels normally requires removal of the spleen (splenectomy).
Whipple’s procedure (pancreatoduodenectomy or pancreaticoduodenectomy)
In this procedure, the surgeon removes the pancreatic head, the duodenum (the first part of the small intestine), part of the jejunum (the next part of the small intestine), the common bile duct, the gallbladder, and part of the stomach (figure 2). It is important to also remove all lymph nodes associated with the pancreas. It may be necessary to remove the major vein running through the pancreas (portal vein).
After removal of these essential organs the intestines are then ‘reconstructed’ to allow the passage of food, bile from the liver and pancreatic digestive juices.
In the past, complications rates were high and death following the Whipple procedure was not uncommon. However, more recent results suggest better outcomes. Better outcomes are more likely in hospitals that perform many Whipple procedures and when the surgeon is experienced with the procedure.
Some centres are now performing laparoscopically assisted or robotically assisted whipped procedure with variable outcomes. The gold standard for this complex operation remains conventional open surgery.
Distal (subtotal) pancreatectomy
Tumours in the body or tail of the pancreas do not cause the same symptoms as those in the head of the pancreas, these cancers tend to be discovered at a later stage, when they are more advanced.
If the tumour looks to be removable on imaging scans, a diagnostic laparoscopy is usually done first to make sure the cancer has not spread. If surgery is an option, left side of the pancreas is removed, usually along with the spleen (splenectomy). Because the small bowel is not disrupted there is often no ‘reconstruction’ required.
Laparoscopically assisted surgery may be performed for left sided tumours with similar outcomes to conventional open surgery, provided the tumour is contained within the pancreas.
Total pancreatectomy - removing the whole of the pancreas may be required if there are multiple tumours in the pancreas, or if a tumour is large and involving the left and right side of the pancreas. Removal of the entire pancreas is associated with diabetes and difficulty in blood sugar control, even with insulin. As such it is only performed when necessary.
Pancreatic drainage procedures – these operations are now rarely performed for chronic pancreatitis. There use is now limited to when endoscopic treatments have failed.
What are the risks of pancreatic surgery?
Up to 40% of patients undergoing complex pancreatic surgery will develop a complication.
Infection - Antibiotics are used around the time of the operation to prevent, chest infection, wound infection, infection in the bile, infections from drips and urine infections. Physiotherapy and getting on your feet early helps a prevent chest infection (pneumonia)
Blood clots - The use of surgical leg stockings and daily injections to thin the blood slightly reduce the risk of a blood clot in the leg or chest (DVT or PE). These are often continued after you go home from hospital.
Leakage of bile, pancreatic or intestinal juice from surgical sites - A surgical drain is used to detect any leakage from your operation site. The major complication of pancreatic surgery is the leakage of pancreatic juice which can require further procedures or an extended stay in hospital.
Bleeding - Major bleeding after your surgery is rare and is usually associated with another complication. However, there may be a need for a blood or iron transfusion after such major surgery.
Bowel or stomach stasis - it is common to experience some constipation after major surgery. It may also take some time to get back to eating, as the stomach may not contract efficiently and it is not unusual to vomit occasionally after eating.
Lack of digestive juices - digestive juices can be replaced with tablets taken at meal times.
Diabetes - diabetes can occur if the remaining pancreas has been scarred by recurrent inflammation because of tumour obstruction.
Death - Death following pancreatic surgery is now very rare but is still real risk. At high-volume surgical centres, mortality rates are 1-2%
How long will I be in hospital?
The expected length of stay for a Whipple procedure between 8-14 days, with the first 1 or 2 days in an intensive care ward.
The expected length of stay for a distal pancreatectomy is 5-7 days, with the first day in a high dependency or intensive care ward.
If complications occur after surgery an extended stay in hospital is likely.
When will I be able to return to normal activity?
After discharge to hospital you will continue to recover from surgery at home. Normal activity and return to work could be expected at 6 weeks. You will be seen in the surgeons’ office at 2 weeks and 6 weeks after discharge.